Retrograde tracheal intubation
Ever wanted to combine a Tuohy needle and an airway procedure?
Well here it is.
In 1960 - inspired by the vascular guidewire techniques we love so much - Drs Butler and Cirillo first intubated a patient by inserting a needle and guidewire into the trachea and out of the mouth, before railroading a tube over it in the conventional direction into the larynx.
This technique has been largely replaced by awake fibreoptic intubation, but that doesn't make it any less cool.
You also need to be able to describe it for exam purposes.
Indications
- Un-intubatable via conventional techniques
- Fibreoptic intubation is going to be prohibitively difficult - excessive secretions or bleeding, airway tumours
Contraindications
- Unconscious patients at risk of aspiration
- Agitated patient
- Coughing
- Cannot identify cricothyroid membrane
- Local uncontrolled infection of the front of the neck
- Severe uncontrolled coagulopathy
- Anatomical pathology making safe cannulation of the trachea infeasible
Complications
- Failure of procedure
- Loss of airway
- Hypoxia
- Trauma
- Bleeding
- False passage
- Laryngospasm
- Subcutaneous emphysema
- Infection
Equipment
There are purpose-built kits available, such as the Cook retrograde intubation kit, however a fairly standard set up would include:
- Chlorhexidine
- 2 ml, 5 ml and 20 ml syringes
- Hypodermic needle for local anaesthetic
- 1% lidocaine with 1:200 000 adrenaline
- 4% lidocaine
- 16G Tuohy needle
- Epidural catheter or guidewire
- Laryngoscope
- Magill's forceps
- Endotracheal tube
- Lubricant
- Artery forceps
- Suction
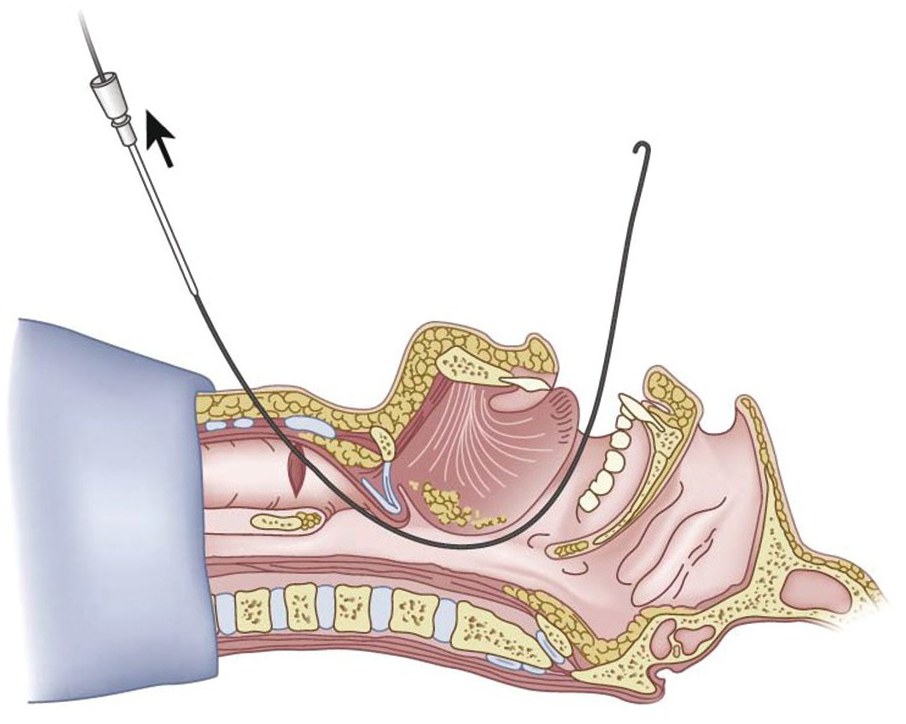
Insertion
- Supine with extended neck
- Clean with chlorhexidine or equivalent
- Identify cricothyroid membrane and laryngeal handshake
- Local anaesthetic with adrenaline to skin over membrane
- Advance needle through membrane and aspirate air to confirm position
- Inject 4% lidocaine to airway at end expiration, to ensure lidocaine is inhaled first before coughing
- Remove needle immediately, before the patient coughs (awake patients only)
- Insert Tuohy needle through cricothyroid membrane, with tip pointing up towards the head
- Aspirate air again to confirm position
- Introduce guidewire or epidural catheter
- Retrieve wire or catheter from mouth using Magill's forceps +/- laryngoscopy (in asleep patient)
- Pull enough wire through to allow endotracheal tube to be railroaded and wire to be grasped at the distal end
- Clamp both ends of the wire
- Hold wire taught and advance endotracheal tube into trachea
- Remove wire by pulling back through the endotracheal tube
- Confirm correct tube position - ETCO2, Ausculatation, chest movement
{kind=link}
For nasal intubation
- Insert suction catheter into nose and retrieve from the pharynx
- After retrieving wire from the pharynx, feed it into the oral end of the suction catheter and out of the nose
- Intubate as above, but via the nose
Never force the needle or wire.
Here's a cadaveric demonstration on YouTube
And here's a less cadaveric demonstration
Here's our airway equipment library
Airway equipment library
Tubes, tips and tricks
 Anaestheasier ltd.
Anaestheasier ltd.