Off-Pump Cardiac Bypass Surgery

Take home messages
- Off-pump surgery involves grafting a new vessel, usually the internal mammary artery, onto the obstructed vessel while the heart is still beating
I'll just let that sink in for a second.
- To do this, the heart is stabilised in the pericardium and the area of interest essentially pinned in place while the rest of the heart continues to beat around it
- Clearly, this can have profound haemodynamic effects that the anaesthetist needs to anticipate and manage
The Surgical Technique
If you do nothing else today, pop the kettle on and watch this insanely cool video on how this whole thing works.
There's also this video on aortic cannulation for 'on-pump' surgery which is interesting.
What are the complications of cardiopulmonary bypass?
- Systemic inflammatory response syndrome
- Consumptive coagulopathy
- Platelet dysfunction
- Stroke and cerebral injury
- Renal injury
What are the two techniques for off-pump bypass surgery?
- Conventional midline sternotomy
- Minimally invasive direct access coronary artery bypass
In the minimally invasive technique, the left internal mammary artery is anastomosed to the LAD via a small anterior left thoracotomy. While less invasive, it only allows one graft to be performed, so is rarely employed.
A bit of history
Off pump surgery has been around since the 1960s, but the invention of bypass rather took over and the off pump techniques took somewhat of a back seat. However since the 1980s there has been more interest in the off-pump option, largely because you avoid all the potential complications of bypass, and it may well be a better option for a certain cohort of patients.


If you're wondering who in the world has the best answer to the question:
"Tell me about a time you dealt with stress"
Well, on February 18, 2012, these guys performed a successful off-pump coronary artery bypass operation on Emperor Akihito.
Yes.
Emperor.
Anaesthetic Techniques
What are the aims for the anaesthetist?
- Cardio-stable induction and maintenance of anaesthesia, avoiding tachycardia
- Haemodynamic stability
- Early extubation and mobilisation
- Good post operative analgesia
- Many places still employ the good old fashioned combination of high dose opioids, volatiles and propofol
- Isoflurane and sevoflurane may have the added benefit of preconditioning the heart muscle against the inevitable intraoperative ischaemia
- Some places use spinal or thoracic epidural anaesthesia as well as GA
What are the benefits of thoracic epidural in this instance?
- Arterial dilatation
- Effective analgesia
- Reduced myocardial oxygen demand
- Earlier extubation
There is not strong data to suggest that thoracic epidural provides meaningful long term benefit over GA alone
- A key aim is to avoid arrhythmias, which is easier said than done, but one can consider giving 5g of magnesium after induction (slowly please) and maintaining potassium above 4.5mmol/litre
Anticoagulation
Every other surgeon: "It's not safe to operative above an INR of 1.4"
Cardiothoracic surgeons: "Give another trillion units of heparin as I make a hole in the aorta"
Heparinisation is usually given prior to dividing the internal mammary artery, and 1–2 mg kg−1 is usually enough and reversal is with protamine.
Haemodynamics
There are three main reasons the blood pressure can be all over the place during handling of the heart:
- It's tilted such that the blood has to flow upwards into the ventricles, needing a greater filling pressure to maintain cardiac output
- The retractors used to hold it in place unsuprisingly restrict the ability of the ventricles to fill effectively
- The change in orientation of the heart can distort the valves and lead to substantial regurgitation
Your aim as the anaesthetist is to maintain a mean arterial pressure above 70mmHg, with a well-filled and preferably slow-beating heart.
Esmolol is your friend here, and you can pace if it's too slow.
Monitoring
Clearly an ECG is going to be less accurate when the heart isn't really in the chest anymore, however you can still detect ischaemia with a 12 lead trace, especially if monitoring the trend of ST elevation over time.
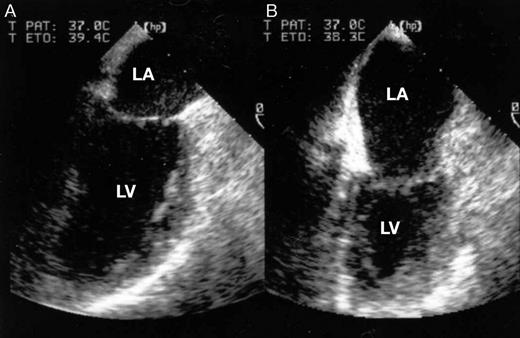
The same applies to trans-oesophageal echocardiography - it usually produces poor images given the heart is being lifted away from the oesophagus, but it can still be of some use, so is often employed given it is fairly low risk as an intervention.
Invasive arterial blood pressure monitoring and central venous catheterisation probably goes without saying.
Oh and remember to say 'AAGBI' or something similar in your viva.
Outcomes
This seems a little contentious.
Previously, it was reported, according to the National Adult Cardiac Surgery Database, that there was a "reduction in risk adjusted mortality from 2.9% in CABG to 2.3%" for off-pump surgery.
Apparently the complication rate was also reduced from 12% to 8%.
However if you read the tweets below, it may not seem so clear cut.
Useful Tweets
Conversion to cardiopulmonary bypass in off-pump CABG
— Sezar (@surgeon_sezar) January 11, 2023
طبعاً العمليات هاي اني ما الي اي دور بيها فقط اتفرج و اصور
الفخر كله لجراحين المركز العراقي لامراض القلب الابطال بكل ما للكلمة من معنى#CABG #coronaryheartdiseases #open_heart_surgery pic.twitter.com/k7NxERCPeY
Sometimes < is not better. In RCT, off-pump bypass surgery way worse than on-pump at 5y (lower survival, more MACE)https://t.co/bIWQBbvoDb pic.twitter.com/PVircrSzPu
— Sek Kathiresan MD (@skathire) August 16, 2017
🚨Guidelines🚨
— Anaesthesia Critical Care & Pain Medicine (ACCPM) (@AccpmJ) May 18, 2022
✨Enhanced recovery after cardiac surgery under cardiopulmonary bypass or off-pump ✨#ERACS 🫀
Accessible in #OpenAccess 👇
🔗https://t.co/UzonsyN3UO#guidelines #cardiacsurgery pic.twitter.com/Z4uldaxlVl
References and Further reading:


Recommended Textbooks:
- CRQs for the Final FRCA - Akuji, Martin, Chambers and Thomas
- CRQs and SBAs for the Final FRCA: questions and detailed answers - Sumner, Allen, Feneley, Raithatha
Revising for the Primary?
Try our free Viva Practice Questions

Everything you need to pass the FRCA Primary
Remember there's a 60% discount on the toolkit for Anaestheasier members, and you get all of our PDFs and Flashcard decks for free too!