Erector Spinae Plane Block
If you're just about to perform the procedure for rib fractures and only need the key refresher points:
- Patient sat up as for a labour epidural
- Ultrasound cranio-caudal at T5*
- Paraspinal - 2-3cm lateral to midline
- Needle can approach from above or below
- Move probe laterally to find rounded rib shadows
- Then move probe medially until rounded shadows become square (transverse processes)
- Pleura should not be easily visible if you're in the right area
- Aim to contact the bone and infiltrate a layer of 20-30ml of local anaesthetic (0.25% levobupivacaine is sensible)
- Can leave a catheter or do a stand alone block
It's generally accepted that you'll get 4 spaces of cover either side of your injection site, so T5 should cover T1-T9
If you just want to watch a video
We would highly recommend you subscribe to @regionalanesthesiology on YouTube - they make incredibly high quality videos and explain techniques very nicely indeed.
Podcast episode
Take home messages
- The ESPB is a simple and highly effective block for debilitating rib fracture pain
- It's also fabulous for postoperative thoracic pain
- It has many other uses as well, including potential for use in obstetrics
A Gratifying moment
One of the greatest feelings in anaesthesia is knowing you have absolved a patient of debilitating pain.
Whether it's seeing a distraught labouring mother finally fall asleep after her epidural starts to work, or the man with excruciating haemorrhoids finally sit comfortably for the first time in six months, regional anaesthesia is the business when it comes to rapidly (and sometimes completely) removing a patient's pain.
I recently had the absolute pleasure of treating the most fabulously eccentric eighty-five year old librarian and feline connoisseur who had been found having taken a tumble at home and fallen against her rocking chair, snapping multiple ribs down her right side and winding her up in a heap in the emergency department.
Needless to say the fentanyl PCA wasn't quite cutting the mustard, and she lay crumpled and breathless in the bed, unable to cough, with a steadily creeping oxygen requirement.
So we consented her for an erector spinae block and trundled her up to theatre.
Within fifteen minutes of sliding the epidural catheter into her back, she was sat up in recovery, tea in hand, nattering contentedly with the recovery staff.
I asked her to cough, whereupon she took a deep breath in and cleared her chest for the first time in hours.
It was magic.
The Erector Spinae Plane block is a safe, reliable and easy-to-learn technique that can not only relieve a patient of agonising rib fracture pain, but potentially save them from a fatal chest infection, so if you're interested - read on.
You Can't Beat NYSORA
When it comes to regional anaesthesia, NYSORA have rather neatly secured the monopoly on producing the best teaching resources, and fair play to them - they're incredible.
They've also very graciously stated that they're happy for their resources to be shared around as long as they are appropriately credited, and of course - everything we share is hyperlinked back to their site, which you should definitely investigate.
- Subscribe to their YouTube channel here
A nice halfway house
Before 2016, if you had painful rib fractures that were deemed in need of regional analgesia, you either received a thoracic epidural or paravertebral block if they were bilateral or multiple, or alternatively an intercostal block if there were just a couple.
However each of these have their issues, whether it's increased systemic absorption of local anaesthetic via an intercostal block, or an epidural being contraindicated by anticoagulation.
The erector spinae plane block (ESPB), however provides a nice compromise of avoiding neuraxial blockade with its risks and contraindications, but still providing wide coverage for multiple rib fractures.
We don't really know how it works
Generally speaking, when you perform a nerve block, and see the cross section of the nerve float up on a flood of injectate, it's easy to appreciate that that is where the drug is having its effect.
But with the erector spinae plane block (ESPB) it's rather less clear.
It might be one or both of the following:
- Local anaesthetic spread along the fascial plane and anaesthetising the posterior rami of the spinal nerves
- Diffusion anteriorly into the paravertebral space with a more central action
But either way, it seems to work well.
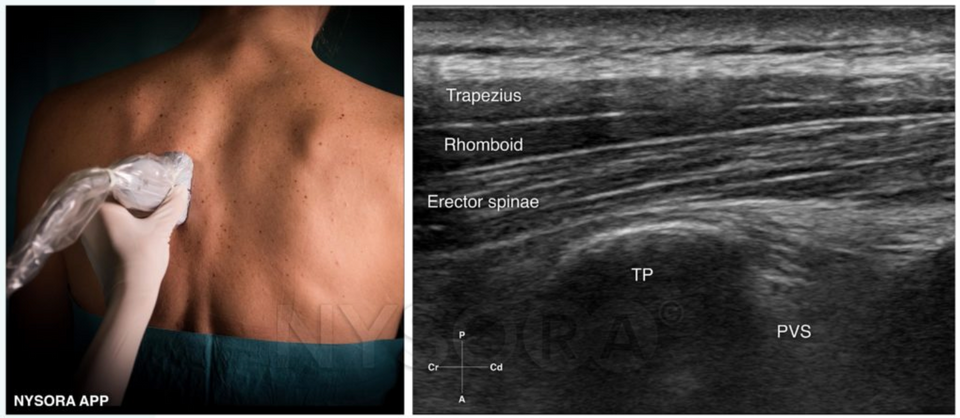
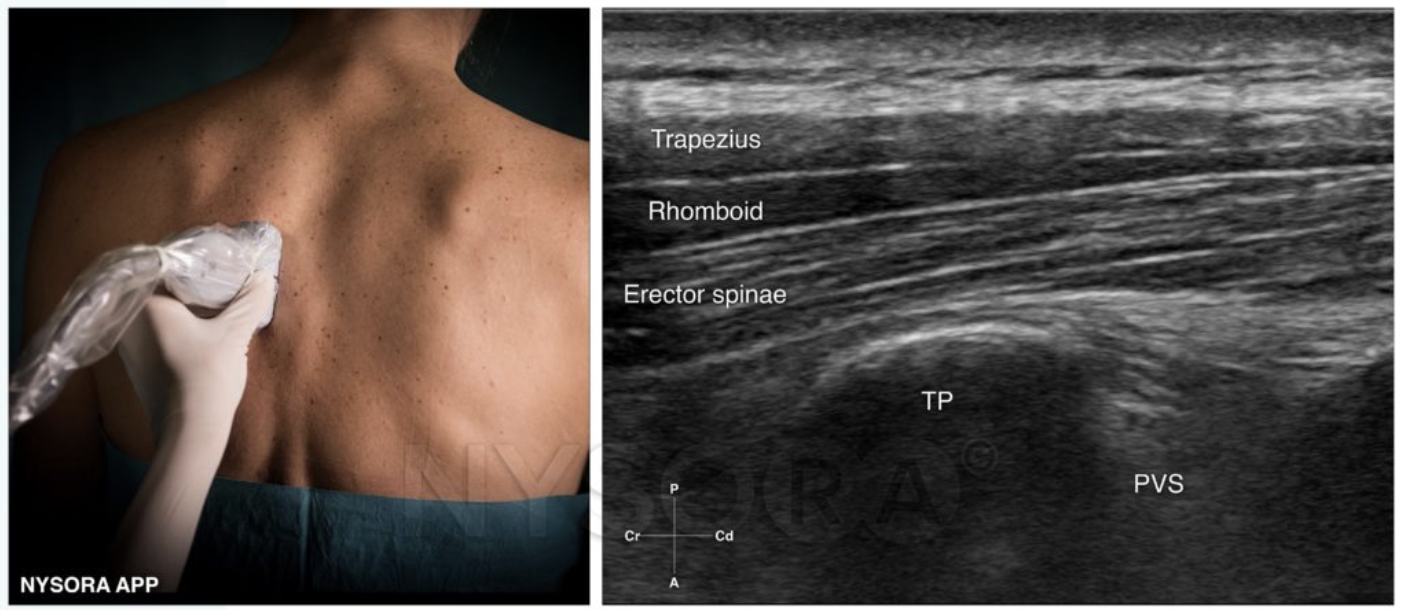
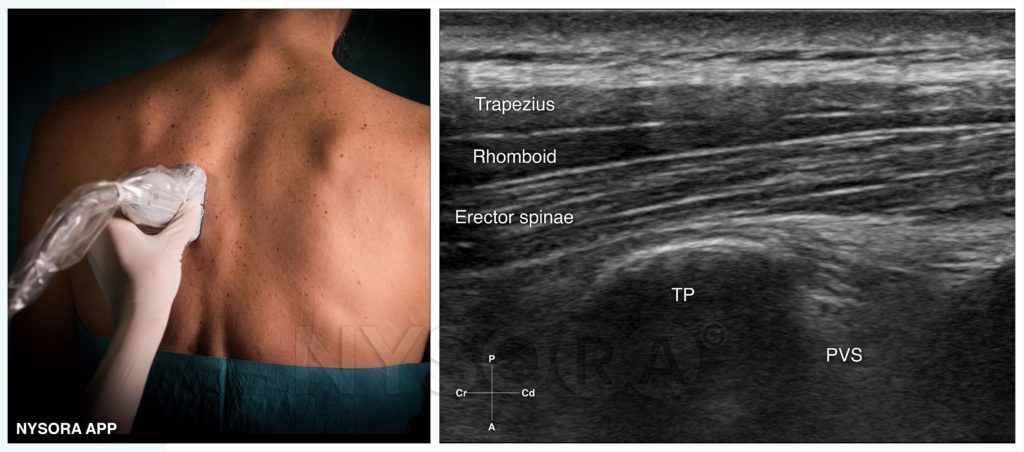
Where to put your probe, and what to look for
The erector spinae is a group of three muscles that runs from skull to sacrum, lying immediately deep to the thoracolumbar fascia.
It arises from the erector spinae aponeurosis, and it plays a vital role in stabilising the spine and posture.
Which muscles form the erector spinae group?
- Longissimus - middle
- Spinalis - medial
- Iliocostalis - lateral
These all have cervical, thoracic and lumbar components.
To find it, simply plonk the probe just off-centre on the thoracic spine, with the probe itself oriented cranio-caudally as in the image above.
Positioning options
- Sitting
- Lateral
- Prone
I generally prefer the sitting position, but whatever works, as long as you can get a decent view!
Slide the probe laterally until you spot nice rounded rib lines, with interspersed hyperechoic pleura.
Then slide medially until these rounded lines turn into square transverse process shadows.
In plane vs Out of Plane
As with anything in anaesthesia, you can do it your own way, as long as it's safe and clinically justifiable.
You can do blocks in plane or out of plane, however most people seem to stick with the in plane approach.
Your needle can approach from above or below, whichever floats your fascial plane.
This way you can see the entirety of the needle as it approaches the transverse process, right up until it makes contact with the bone.
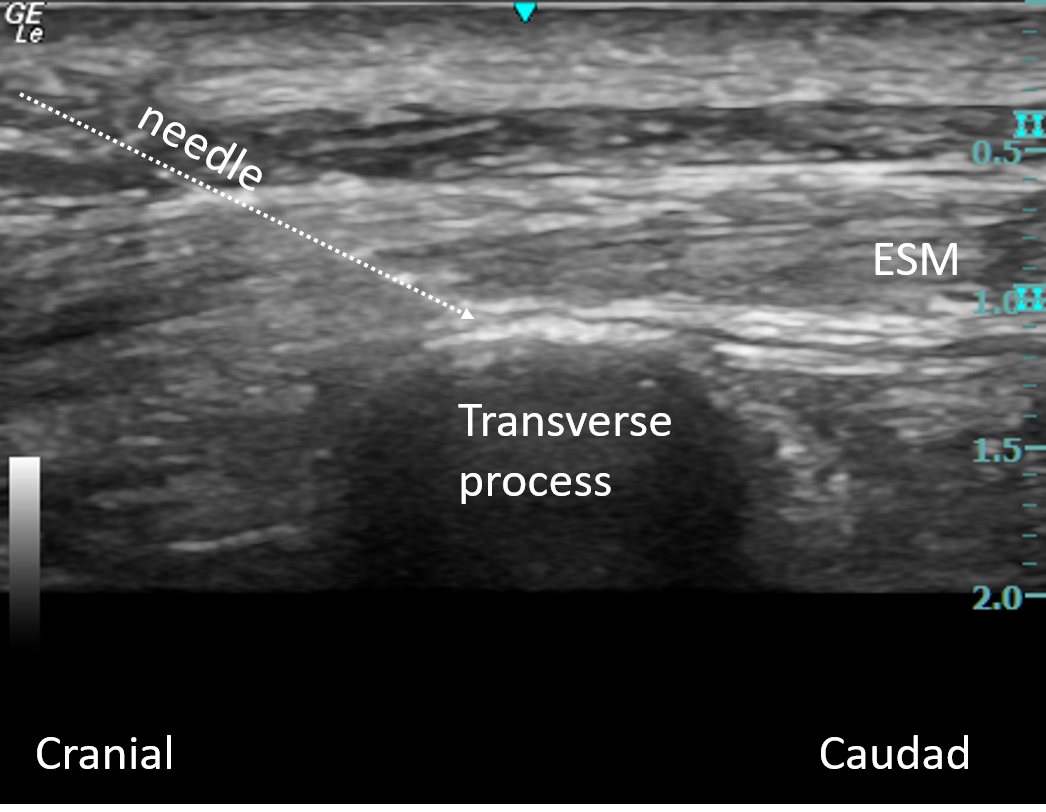
Then aspirate the needle to ensure you're not in a blood vessel or the pleura, and inject a few millilitres to visualise the spread of anaesthetic deep to the erector spinae muscle.
Once you're happy with how the image looks, you can give the whole 20-30mls, and insert the catheter if you're planning on leaving one in situ.
Options for catheters:
- Specific nerve block catheter kit (cannula over needle technique)
- Standard epidural kit (Tuohy needle)
It has other uses too
These clever people reckon it could even act as understudy for the epidural for labour analgesia, when neuraxial blockade is relatively contraindicated:
🔐The erector spinae plane block for obstetric analgesia: a case series of a novel technique.
— 𝘈𝘯𝘢𝘦𝘴𝘵𝘩𝘦𝘴𝘪𝘢 𝘙𝘦𝘱𝘰𝘳𝘵𝘴 (@Anaes_Reports) November 25, 2020
This new report from @VilchisSalvador and @DrPhilipPeng is now #FreeForAWeek!
🔗https://t.co/BKetv4SDdU pic.twitter.com/9ByKnZ6Kb9
Useful Tweets and Resources
From NYSORA's Nerve Blocks App News: Tips for the Erector Spinae Plane Block! Which case did you use an erector spinae plane block for most recently? Let us know!
— NYSORA (@NYSORA) March 21, 2023
Check out our walkthrough here in the Nerve Blocks app: https://t.co/wks1RQzQ7n pic.twitter.com/tTNG390KZy
For a discussion on “Chuff Levels”, Plus some tips and tricks on the Erector Spinae Plane block, tune in to @BlockIt_Hot_Pod #BlockItLikeItsHot Episode 2!
— Dr Amit Pawa (@amit_pawa) December 15, 2022
We thought we’d start off talking about something “slightly controversial”!
Tune in via your usual podcast provider! pic.twitter.com/rSdEET6WO0
Clavicle surgery with contraindications to a thoracic epidural?
— 𝘈𝘯𝘢𝘦𝘴𝘵𝘩𝘦𝘴𝘪𝘢 𝘙𝘦𝘱𝘰𝘳𝘵𝘴 (@Anaes_Reports) May 8, 2023
Consider bilateral erector spinae plane blocks!@suryatheja10 @drnishkarsh @drnaveen1984 @RegionalAnaesUK #FreeForAWeekhttps://t.co/y2DKQpdZWJ pic.twitter.com/o0c00VGMzs
🔓PROSPECT guideline for elective caesarean section: an update.
— 𝘈𝘯𝘢𝘦𝘴𝘵𝘩𝘦𝘴𝘪𝘢 (@Anaes_Journal) May 2, 2023
"...the PROSPECT group now recommends erector spinae plane block for analgesia after caesarean section, as an alternative to long-acting neuraxial opioids."
🔗https://t.co/ZTNHGN4Lbf pic.twitter.com/b8AbMExDN1
References and Further Reading



Free Question Bank
The marvelous crew over at frca-revision.com have kindly given us permission to share their fabulous new question bank - tap the image and go check it out!
Primary FRCA Toolkit
While this subject is largely the remit of the Final FRCA examination, up to 20% of the exam can cover Primary material, so don't get caught out!
Members receive 60% discount off the FRCA Primary Toolkit. If you have previously purchased a toolkit at full price, please email anaestheasier@gmail.com for a retrospective discount.

Discount is applied as 6 months free membership - please don't hesitate to email Anaestheasier@gmail.com if you have any questions!
Just a quick reminder that all information posted on Anaestheasier.com is for educational purposes only, and it does not constitute medical or clinical advice.